Autism Spectrum Disorder (ASD) is a complex neurodevelopmental condition that significantly affects how individuals interact with others, communicate, learn, and behave. Far from being a singular condition, ASD encompasses a broad range of presentations and support needs, hence the term “spectrum.” For Registered Behavior Technicians (RBTs), understanding the nuances of ASD is paramount to delivering effective, evidence-based interventions.
For families, gaining a comprehensive understanding is crucial for navigating diagnosis, accessing appropriate support, and fostering their child’s development and well-being. This guide aims to bridge the knowledge gap, offering essential insights for both professional caregivers and the families they support.
Understanding the Spectrum: Variability and Diagnostic Criteria
Autism is a lifelong condition rooted in differences in brain development. The clinical definition, as outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), characterizes ASD by persistent deficits in social communication and social interaction across multiple contexts, alongside restricted, repetitive patterns of behavior, interests, or activities. These symptoms must be present in the early developmental period, though they may not become fully apparent until social demands exceed an individual’s capacities or may be masked by learned strategies in later life.
Defining the Spectrum and Levels of Support
The “spectrum” nature of autism means that each person with ASD has a unique combination of strengths and challenges. This variability is reflected in the DSM-5-TR’s classification of support needs into three levels:
- Level 1: Requiring Support – Individuals may have difficulty initiating social interactions, show atypical or unsuccessful responses to social overtures, and exhibit inflexibility of behavior causing significant interference with functioning.
- Level 2: Requiring Substantial Support – Individuals often have marked deficits in verbal and nonverbal social communication skills, demonstrate restricted interests, repetitive behaviors, or difficulty coping with change, which are obvious to a casual observer.
- Level 3: Requiring Very Substantial Support – Individuals have severe deficits in verbal and nonverbal social communication skills, often with limited intelligible speech, and display extreme difficulty coping with change or highly restricted, repetitive behaviors that markedly interfere with functioning in all spheres.
It is important to recognize that ASD can present differently across various demographics. For instance, research indicates that girls are diagnosed four times less often than boys, partly because their symptoms may be more subtle, with fewer overt social and communication challenges or repetitive behaviors, leading to underdiagnosis or misdiagnosis. Similarly, adults may learn to “mask” their autistic traits, making diagnosis challenging in later life. An individual’s needs, strengths, and challenges may also evolve throughout their life stages, from childhood to adolescence and adulthood, necessitating adaptable support.
Core Diagnostic Features: Social Communication and Interaction
The first core domain of ASD involves significant challenges in social communication and interaction, manifesting in several key areas:
- Deficits in Social-Emotional Reciprocity: This can range from an abnormal social approach and failure of normal back-and-forth conversation to reduced sharing of interests, emotions, or affection, and difficulty initiating or responding to social interactions.
- Deficits in Nonverbal Communicative Behaviors: Individuals may exhibit poorly integrated verbal and nonverbal communication, abnormalities in eye contact and body language, or difficulties understanding and using gestures. This can include an aversion to maintaining eye contact or a lack of proficiency with non-verbal gestures.
- Deficits in Developing, Maintaining, and Understanding Relationships: This includes difficulties adjusting behavior to suit various social contexts, challenges in sharing imaginative play or making friends, and sometimes an apparent absence of interest in peers. Communication challenges can manifest as delayed language development, stilted or scripted speech, and difficulty understanding figurative language or sarcasm.
Core Diagnostic Features: Restricted, Repetitive Behaviors, and Interests
The second core domain involves restricted, repetitive patterns of behavior, interests, or activities, which must include at least two of the following:
Prepare the right way, before your competency assessment.
- Stereotyped or Repetitive Motor Movements, Use of Objects, or Speech: This can include simple motor stereotypies (e.g., hand flapping, rocking, spinning), lining up toys or flipping objects, echolalia (repeating words or phrases), or idiosyncratic phrases.
- Insistence on Sameness, Inflexible Adherence to Routines, or Ritualized Patterns of Verbal or Nonverbal Behavior: Individuals may experience extreme distress at small changes, have significant difficulties with transitions, exhibit rigid thinking patterns, or insist on specific greeting rituals or routes. These routines provide predictability and reduce anxiety.
- Highly Restricted, Fixated Interests that are Abnormal in Intensity or Focus: This might involve a strong attachment to or preoccupation with unusual objects, or excessively circumscribed or perseverative interests. While these intense interests can be a source of motivation, they can also limit social interactions if they become all-consuming.
- Hyper- or Hyporeactivity to Sensory Input or Unusual Interests in Sensory Aspects of the Environment: This is a crucial, often misunderstood, component.
Sensory Processing Differences: An Integral Aspect
Sensory processing differences are a common and significant feature of ASD, experienced by an estimated 90% of individuals with the condition. These differences are specifically noted in the DSM-5-TR as one of the four categories for restricted and repetitive behaviors, interests, or activities. Individuals with ASD may be hyper-sensitive (over-responsive) or hypo-sensitive (under-responsive) to sensory input across various senses, or even within the same sense.


- Hyper-sensitivity: This means being overly responsive to certain sensory stimuli. Examples include extreme aversion to loud noises, bright lights (e.g., fluorescent lighting), specific textures (e.g., clothing fabrics, certain foods), strong smells, or unexpected touch. These triggers can lead to sensory overload, causing significant distress, anxiety, or behavioral outbursts.
- Hypo-sensitivity: This refers to being under-responsive to sensory stimuli, leading individuals to seek out more input. Examples include a high pain tolerance, seeking intense pressure (e.g., weighted blankets), a fascination with lights or movement, or excessive smelling or touching of objects.
These sensory processing differences profoundly impact daily functioning, learning, and emotional regulation. Environments that neurotypical individuals find unremarkable, such as a busy shopping center or a brightly lit classroom, can be overwhelming for someone with ASD. Understanding an individual’s unique sensory profile is essential for providing effective support and creating accommodating environments.
Navigating Diagnosis and Early Intervention
Early identification and intervention are critical for improving outcomes for individuals with ASD. Signs of ASD can sometimes be noticed by parents or pediatricians as early as 18 months of age or younger. By age two, a diagnosis from an experienced professional can be considered reliable, though many children do not receive a final diagnosis until much later, sometimes in adolescence or even adulthood. Delayed diagnosis means lost opportunities for early support, which can significantly improve a child’s functioning.
The Diagnostic Journey and Timelines
The diagnostic process typically begins with parental or caregiver concerns shared with a pediatrician, who monitors developmental milestones. If concerns arise, a specialized evaluation is recommended, involving developmental pediatricians, pediatric psychologists, child neurologists, or child and adolescent psychiatrists. This evaluation includes structured observations, interactions with the child, and interviews with caregivers. For children under three, evaluations can be accessed through local early intervention systems. For those over three, local schools can provide evaluations, even if the child is not yet enrolled.
Importance of Early Intervention and Co-occurring Conditions
Once diagnosed, individualized treatment plans are crucial. These plans often involve multiple professionals and aim to reduce symptoms that interfere with daily functioning and quality of life. Current research, supported by institutions like the National Institute of Mental Health (NIMH), focuses on improving early screening and providing appropriate services and supports as early as possible.
It’s also important to note that many individuals with ASD experience co-occurring conditions, which require concurrent treatment. These frequently include attention-deficit/hyperactivity disorder (ADHD), anxiety, depression, intellectual disability, gastrointestinal disorders, seizures, and sleep disorders. Treating these conditions alongside ASD-specific interventions is vital for comprehensive care and improving overall well-being.

The Role of Registered Behavior Technicians (RBTs) in Supporting Individuals with ASD
Registered Behavior Technicians (RBTs) play a vital role in the implementation of Applied Behavior Analysis (ABA) interventions, which are widely recognized as evidence-based for individuals with ASD. RBTs work directly with clients under the supervision of a Board Certified Behavior Analyst (BCBA), applying behavioral principles to teach new skills and reduce challenging behaviors.
Foundations of Applied Behavior Analysis (ABA)
ABA therapy involves the systematic study of functional challenges to create structured behavioral plans. Its core principles focus on understanding how behavior works in real-life situations, how the environment affects behavior, and how learning takes place. ABA programs are highly individualized, targeting observable, measurable behaviors to improve adaptive skills and decrease inappropriate behaviors. The goal is always to enhance the individual’s quality of life and promote independence. Effective ABA practices utilize various techniques such as positive reinforcement, where desired behaviors are rewarded to increase their likelihood of future occurrence. Prompting strategies guide individuals toward correct responses, and then prompts are systematically faded to promote independence. Task analysis breaks down complex skills into smaller, manageable steps, facilitating learning through sequential mastery.
Practical Strategies for RBTs: Skill Acquisition and Behavior Reduction
RBTs are directly responsible for implementing the behavior intervention plans designed by BCBAs. This requires consistency, precision, and an understanding of each client’s unique needs. For example, when addressing self-injurious behaviors, an RBT would meticulously collect data, apply differential reinforcement of alternative behaviors (rewarding desired behaviors while ignoring or redirecting problematic ones), and implement communication training to help the individual express their needs in a more appropriate way. Integrating an individual’s intense or special interests into learning activities can also be a highly effective strategy to aid transitions, reduce anxiety, and promote engagement. For instance, if a child is fixated on outer space, an RBT might incorporate space-themed visuals or narratives into academic tasks or transition cues.
Enhancing Communication and Social Skills
A primary focus for RBTs is to improve communication and social interaction skills.
- Communication Training: Goals can range from developing foundational pre-language skills, such as making eye contact, using gestures (e.g., pointing), and imitating sounds, to teaching more advanced conversational skills like turn-taking, staying on topic, and understanding the nuances of language. This might involve using visual supports, picture exchange communication systems (PECS), or speech-generating devices for nonverbal individuals.
- Social Skills Development: RBTs use structured approaches like social skills training, modeling appropriate behavior, and role-playing to help individuals learn to navigate social situations. This involves teaching them to interpret social cues (facial expressions, body language), understand different emotions, and practice initiating and maintaining friendships. The aim is to reduce social isolation and promote meaningful connections.
Addressing Sensory Challenges in Practice
Given the prevalence and impact of sensory processing differences, RBTs must incorporate strategies to manage sensory input.

- Understanding Sensory Profiles: RBTs work to understand each client’s unique sensory sensitivities (hyper- or hypo-reactivity) through observation and communication with families and BCBAs. This understanding informs environmental modifications.
- Environmental Modifications: Strategies include adjusting lighting, reducing auditory input (e.g., using noise-canceling headphones), creating quiet spaces, or modifying textures in the immediate environment.
- Sensory Tools: RBTs can strategically introduce and teach the use of sensory items such as fidget toys, weighted blankets or vests (with professional guidance), or chewing tools to help individuals regulate their sensory experiences, prevent overload, or meet sensory seeking needs. The consistent and appropriate use of these tools can significantly support an individual’s ability to focus and participate in therapeutic activities and daily routines.
Empowering Families: Strategies for Support and Advocacy
The family is central to support and serves as the basis of the success of a loved one with ASD. The successful involvement of families is essential to outcomes. Empowerment of Families means that families are equipped with the knowledge, resources, and strategies they need to provide support for their loved one with ASD.
Becoming an Informed Advocate
To become an informed advocate for your child with ASD, family members will want to gain as much information as possible to help. Family members are encouraged to understand ASD, what it means to be diagnosed with ASD, what are the strengths of their child, what are their unique challenges in school, how do they want to support their child in particular through educational opportunities, what is available in terms of intervention options, and what other families have done that has been successful or unsuccessful in supporting their child.
Families are the primary advocate for the needs of their child, whether in the education, medical, or recreational/specialty setting. Understanding your family member’s rights to an education, inclusive services, assessment, and treatment is critical to achieving success.
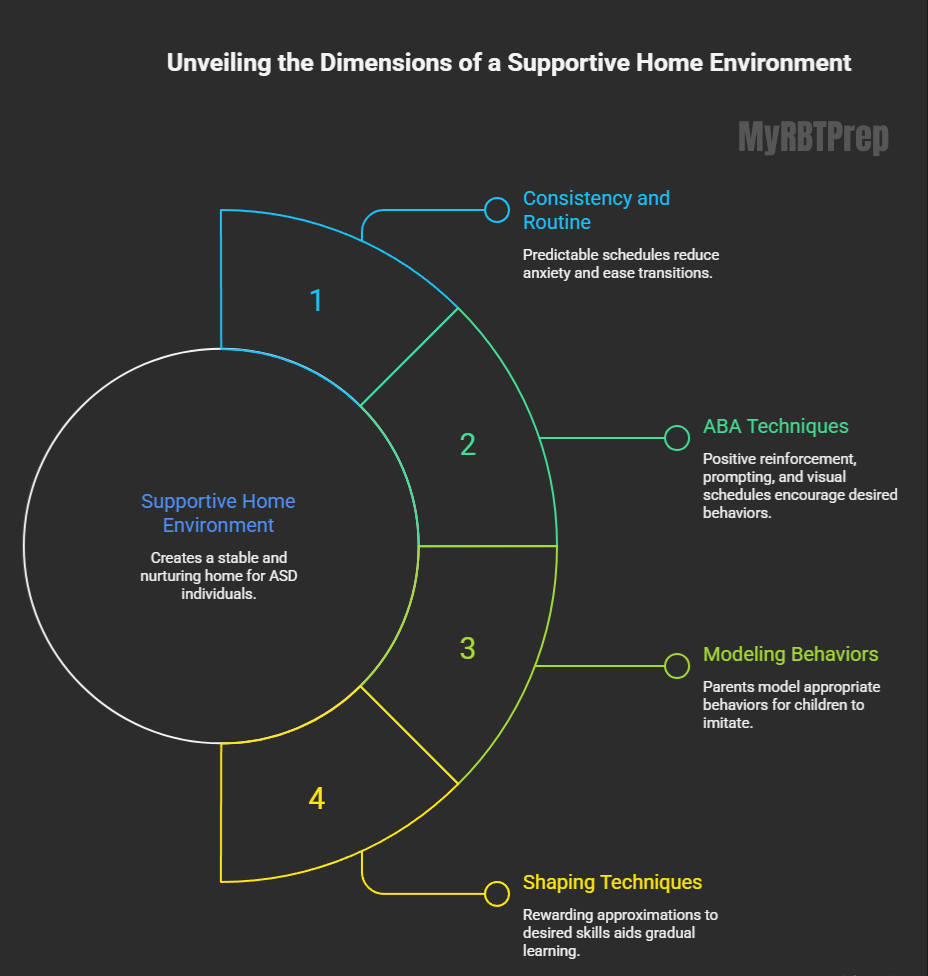
Creating a Supportive Home Environment
A supportive home environment for a family member by providing consistency and routine. Establishing predictable schedules and clear expectations will help your loved one anticipate transition and reduce anxiety. Parents can also use ABA (Applied Behaviour Analysis) strategies to effectively model positive behaviour, positively reinforce positive behaviours, prompt appropriate behaviour, and provide visual schedules to support learning the skills that your family member has learned through therapy. Another powerful tool for parents to use to shape behaviour is to model behaviour that your family member can imitate. Finally, parents can use shaping techniques to provide reinforcement for the closer approximation to a desired skill.
Conclusion: A Lifelong Journey of Growth and Support
Autism Spectrum Disorder is a journey, not a destination. It is a lifelong condition where needs, strengths, and challenges can evolve over time. For RBTs, continuous learning, ethical practice, and individualized, evidence-based intervention remain paramount. For families, informed advocacy, a supportive home, and strong community connections are essential. By working together, RBTs and families can foster environments where individuals with ASD are understood, supported, and empowered to reach their fullest potential, embracing their unique perspectives and contributions to the world.
Frequently Asked Questions (FAQs)
- What is Autism Spectrum Disorder (ASD) according to current guidelines?
ASD is a complex, lifelong neurodevelopmental condition characterized by persistent challenges in social communication and restricted, repetitive behaviors. - How does the “spectrum” in Autism Spectrum Disorder affect needed support?
The spectrum reflects varied support needs, classified into Levels 1, 2, or 3 based on the severity of symptoms interfering with daily functioning. - What is the core responsibility of an RBT working with an individual with ASD?
RBTs implement evidence-based interventions, primarily Applied Behavior Analysis (ABA), to teach adaptive skills and reduce challenging behaviors under BCBA supervision. - What foundational strategy should families prioritize for a supportive home environment?
Families should prioritize providing consistent structure and routine while actively learning about ASD to support generalization of therapeutic gains. - Are sensory differences a significant factor in understanding Autism presentation?
Yes, sensory processing differences (hyper- or hypo-reactivity) are commonly observed and are included as a criterion for the diagnosis of ASD.